AI in Cervical Cytology: What the Evidence Shows, and What It Doesn't Yet
A new open-access narrative review in Diagnostics (MDPI) maps how artificial intelligence is being applied across cervical cancer screening, triage, and diagnosis — and is candid about the limitations that still stand between promising results and routine clinical use.
Cervical cancer is the fourth most commonly diagnosed cancer in women worldwide and the fourth leading cause of cancer death, accounting for roughly 600,000 new cases and over 300,000 deaths each year. The burden falls hardest on low- and middle-income countries, where access to screening, HPV vaccination, and timely treatment is often limited.
A new open-access review in Diagnostics (MDPI) examines how artificial intelligence is being brought to bear on this problem:
Published on 19 May 2026 in the journal’s Machine Learning and Artificial Intelligence in Diagnostics section, the paper was written by a team of nine researchers from institutions in Poland, Japan, and Sweden, with Piotr Religa of the Karolinska Institute as corresponding author.
The clinical context
In contemporary screening programs, HPV testing has largely replaced cytology as the primary screening method, in line with WHO guidance. Cytology’s role has shifted to triage: deciding which HPV-positive women need further investigation. That work is labor-intensive — a single slide can contain thousands of cells — and is subject to inter-observer variability and a shortage of trained cytologists in many regions. These are precisely the pressures that have drawn attention to automation.
The authors are explicit that this is a narrative review, not a systematic one: the literature was selected from PubMed, Scopus, and Web of Science based on the authors’ expertise and relevance, rather than a predefined protocol. It is intended as an accessible map of the field, not a formal meta-analysis.
What the review covers
The paper traces AI applications across the cervical cancer diagnostic pathway:
- Automated and assisted slide screening — systems that flag abnormal areas or cells for cytopathologist review, including the FDA-cleared Genius Digital Diagnostics System and several CE-marked tools.
- Liquid-based cytology — deep learning models that classify whole-slide images as neoplastic or non-neoplastic.
- ASC-US risk stratification — models that triage equivocal cytology results to identify women at higher risk of CIN2+ lesions.
- HPV-positive triage — multimodal approaches combining cytology, HPV testing, and clinical data to reduce unnecessary colposcopy referrals.
- Colposcopy support — systems that assist lesion grading and biopsy targeting.
What the evidence shows — and how to read it
Across these settings, AI-assisted systems have produced encouraging results, but the review is careful to present them as ranges drawn from very different studies rather than a single headline figure. In the performance synthesis (Table 2), reported sensitivity spans roughly 72% to 99% and AUC values 0.74 to 0.99, depending on the application, dataset, and reference standard.
A few illustrative findings:
- In a multicenter observational study of referral women, AI-assisted reading detected 92.6% of CIN2 and 96.1% of CIN3+ lesions — equivalent sensitivity and higher specificity than skilled cytologists in that setting.
- An AI microscope study reported sensitivity for LSIL+ detection rising from 86.0% to 95.0%, with improved agreement between cytopathologists.
- In ASC-US triage, one DL model showed higher sensitivity (92.9% vs. 89.3%) and specificity (49.7% vs. 34.3%) than hrHPV testing, at no added cost.
- AI-assisted triage of HPV-positive women reduced colposcopy referrals by 10–20 percentage points in several studies.
The authors stress repeatedly that these numbers should not be compared head-to-head. As Table 2 notes, the figures “are not derived from head-to-head comparative evaluations,” and differences may reflect study design, prevalence, and reference standards rather than true differences between systems. Much of the evidence comes from retrospective, single-center, or enriched datasets and referral populations — not routine primary screening — so reported gains cannot be assumed to carry over to real-world HPV-primary programs.
The barriers that remain
The review devotes substantial attention to what stands between these results and routine clinical use:
- Data. Robust models require large, diverse, standardized datasets with ground-truth diagnoses, which remain scarce.
- Validation. Many models have been evaluated only retrospectively; of nearly 300 FDA-approved AI medical devices, only a small fraction have been tested in prospective randomized trials. Reporting standards such as the CONSORT-AI extension are still being adopted.
- Regulation. Only one FDA-approved AI tool currently exists for cervical cytology (Hologic Genius), though at least three systems have recently been CE-IVD approved in Europe, where certification under the IVDR is more decentralized.
- Infrastructure. AI in cytology presupposes digital cytology infrastructure — scanners, storage, and computation — a significant up-front investment, especially in the resource-limited settings that stand to benefit most.
- Ethics and accountability. Open questions remain about liability for misdiagnosis, the “black box” nature of many models, and what informed consent means when the rationale for a diagnosis is opaque.
Conclusion
The review’s overall position is measured:
“AI should therefore be regarded as a promising adjunct to human expertise rather than a replacement in cervical cytology and related clinical diagnostic pathways.”
That conclusion — that AI’s near-term value lies in augmenting cytopathologists and cytotechnologists, particularly where human resources are stretched, rather than replacing them — reflects the framing that runs throughout the paper.
A note on Scanome’s involvement
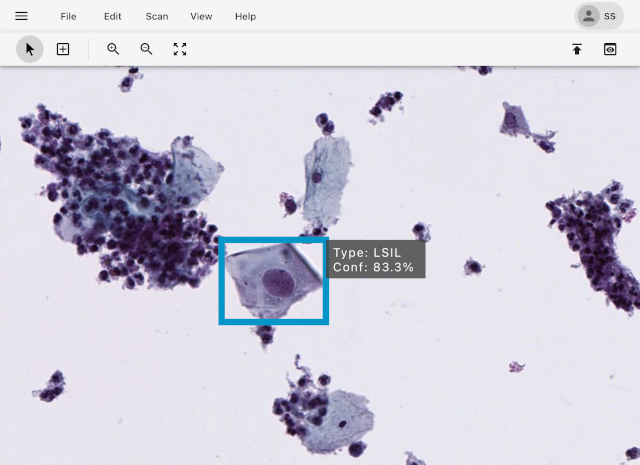
Scanome’s ScanAI Viewer appears as Figure 1 in the paper, illustrating a real-world cervical cytology AI interface in which detected dysplastic cells are ranked by probability of dysplasia for diagnostic review and quality control. As the authors disclose in the paper, ScanAI is a commercial product, Piotr Religa is the owner of Scanome Ltd., and the figure is included solely for illustrative purposes. We mention it here in the same spirit.
Open access
The full article is freely available under a Creative Commons license.
DOI: 10.3390/diagnostics16101541
Journal: Diagnostics 2026, 16(10), 1541
You can read more about our work on the ScanAI Digital Pathology Platform.